
A 55-year-old woman goes to her primary care doctor because of palpitations, diaphoresis, continued sweating, and feeling nervous. Her physical examination is normal except for elevated heart rate (about 100 beats/min) and blood pressure (150/90 mm Hg). Lab tests show an increased thyroxine level, suggesting an overactive thyroid. She returns for a follow-up visit for palpitations, and a 12-lead ECG is obtained.
Discussion
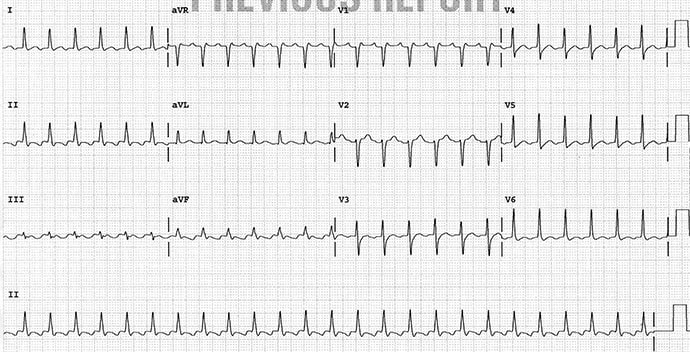
The rhythm is regular, at a rate of 150 beats/min. The QRS complex duration is normal (0.08 sec) with normal morphology. The axis is normal between 0° and +90° (positive QRS complex in leads I and aVF). The QT/QTc intervals are normal (280/440 msec).
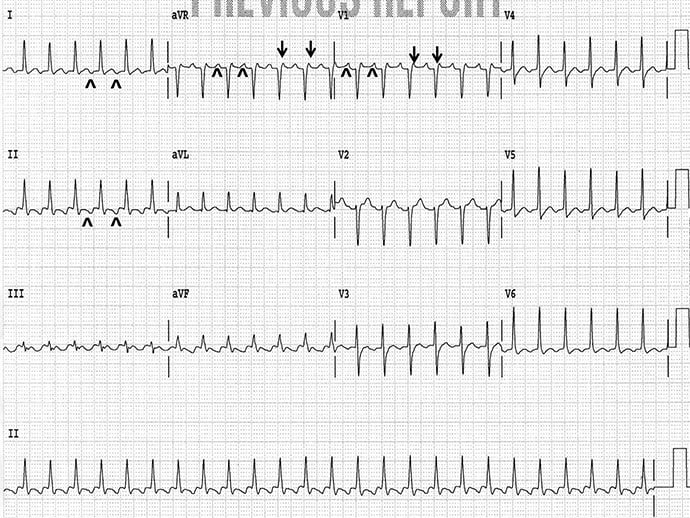
Prominent atrial waveforms occur before each QRS complex (^); they are negative in leads I and aVF and positive in leads aVR and V1 (^). A second atrial waveform is superimposed at the end of each QRS complex — it is most obvious in leads aVR and V1 (↓). The two atrial waveforms have the same morphology and occur at a regular rate of 300 beats/min. Therefore, the rhythm is atrial flutter with 2:1 AV block. Importantly, the only supraventricular rhythm with an atrial rate > 260 beats/min (up to 320 beats/min) is typical atrial flutter.
Philip Podrid, MD, is an electrophysiologist, a professor of medicine and pharmacology at Boston University School of Medicine, and a lecturer in medicine at Harvard Medical School. Although retired from clinical practice, he continues to teach clinical cardiology and especially ECGs to medical students, house staff, and cardiology fellows at many major teaching hospitals in Massachusetts. In his limited free time, he enjoys photography, music, and reading.
